Sepsis
Kenneth Baillie
Roslin Institute, University of Edinburgh
Intensive Care Unit, Royal Infirmary Edinburgh
#References
- Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. Lancet 2010;376:1339-1346
- Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009;302:2323-2329
- Singer et al JAMA. 2016 Feb 23; 315(8): 801–810.
- Bone RC, Balk RA, Cerra FB, et al. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20(6):864–874
- Singer et al JAMA. 2016 Feb 23; 315(8): 801–810.
- Shankar-Hari et al JAMA. 2016 Feb 23;315(8):775-87.
- Shankar-Hari et al JAMA. 2016 Feb 23;315(8):775-87.
- Seymour et al JAMA. 2016;315(8):762-774.
- Marshall J. Trends in Molecular Medicine. Volume 20, Issue 4, April 2014, Pages 195-203
- Pool et al. Critical Care Clinics. 34(1), Pages 63-80 (2018)
# Incidence
- 19 million cases worldwide per year
Adhikari NK, Fowler RA, Bhagwanjee S, Rubenfeld GD. Critical care and the global burden of critical illness in adults. Lancet 2010;376:1339-1346
# Pathogens
## Of patients with severe sepsis who had positive cultures:
- gram-negative bacteria: 62% (*Staphylococcus aureus* and *Streptococcus pneumoniae*)
- gram-positive bacteria: 47% (*Escherichia coli*, *Klebsiella*, and *Pseudomonas aeruginosa*)
- fungi: 19%
Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009;302:2323-2329
# Sources
- Lungs: 64% of infections
- Abdomen: 20%
- Bloodstream: 15%
- Renal tract/genitourinary system: 14%
Vincent JL, Rello J, Marshall J, et al. International study of the prevalence and outcomes of infection in intensive care units. JAMA 2009;302:2323-2329
# Science
* You can't understand an entity until you can:
+ Define it
+ Measure it
# Sepsis
* Life-threatening organ dysfunction caused by a dysregulated host response to infection.
Singer et al JAMA. 2016 Feb 23; 315(8): 801–810.
# Infection
* Your doctor thinks you have an infection
# Organ dysfunction
* Definable and measurable
# Organ dysfunction
## Systemic inflammatory response syndrome (SIRS)
- Heart rate >90/min
- Respiratory rate >20/min or PaCO2 <32 mm Hg (4.3 kPa)
- Temperature >38°C or <36°C
- White cell count >12e3/mm3 or <4e3/mm3 or >10% immature bands
Bone RC, Balk RA, Cerra FB, et al. American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference: definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit Care Med. 1992;20(6):864–874
# Organ dysfunction
## qSOFA
- Hypotension SBP < 100mmHg
- Glasgow Coma Scale (GCS) below 15
- Tachypnoea > 22/min
Singer et al JAMA. 2016 Feb 23; 315(8): 801–810.
Life-threatening Organ dysfunction
## Predictive validity
- *not* an attempt to predict mortality
- an quantitative test for the definition
Life-threatening Organ dysfunction
## Septic shock
- hypotension requiring vasopressors to maintatin mean BP > 65 mm Hg
AND
- serum lactate level > 2 mmol/L
Life-threatening Organ dysfunction
## Mortality
- 10-fold variation for in-hospital mortality across deciles of baseline risk
Seymour et al JAMA. 2016;315(8):762-774.
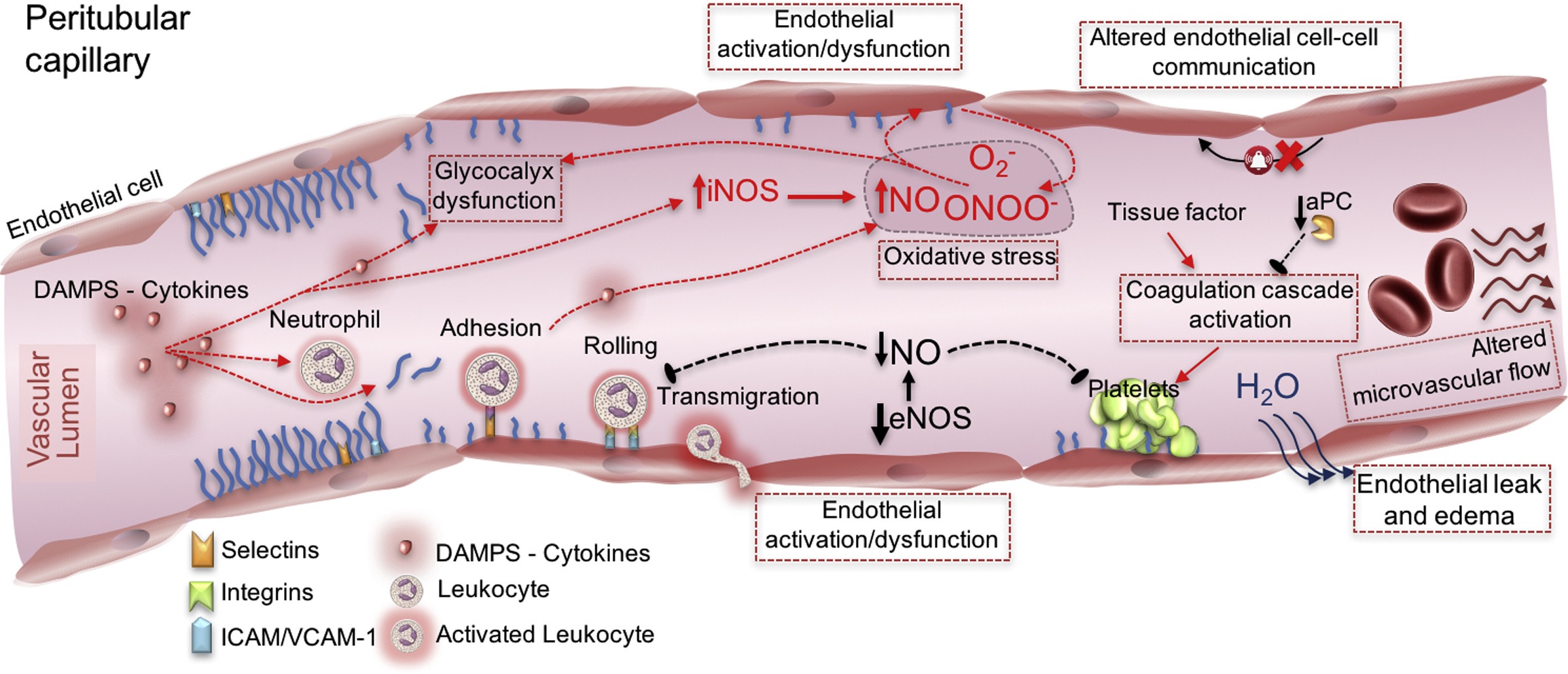
# Sepsis pathophysiology
- hypoxia/ischaemia
Physiological mechanisms of hypoxia
| Utilisation in |
|||||
| Hypoxic gas | |||||
| Type II RF | |||||
| Type I RF | |||||
| Stagnant | |||||
| Cytotoxic |
# Sepsis pathophysiology
- hypoxia/ischaemia; mitochondrial failure
- "cytokine storm"
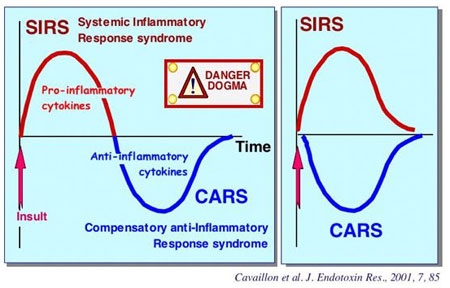
# Sepsis pathophysiology
- hypoxia/ischaemia; mitochondrial failure
- "cytokine storm"
- inflammatory cell recruitment
- endothelial permeability
# Treatment
- Antimicrobials
- Source control
# Treatment: Supportive care
- Intravenous fluid (e.g. balanced crystalloid)
- Vasopressors (e.g. noradrenaline)
- Mechanical ventilation
- Sedation
- Renal replacement therapy
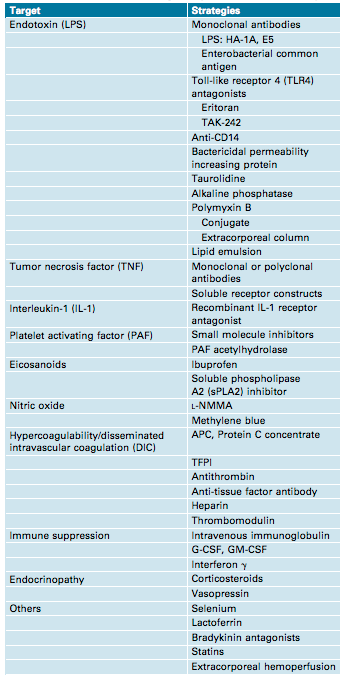
# Treatment: specific interventions to modify pathogenesis
# Treatment failures
- Activated protein C
- Anti-endotoxin antibodies
- Anti-TNF antibodies
FEAST TRIAL
Guidelines: 60ml/kg
Intervention: 20-40ml/kg
1400-2800mls over 1hr for a 70kg patient.
Maitland et al. N Engl J Med 2011; 364:2483-2495Variation in susceptibility to infection is strongly genetic
- 6 - Environment Inherited
- 5 -
- 4 -
- 3 -
- 2 -
- 1 -
- Cardiovascular
- Cancer
- Infection




- Python, R, scipy, networkx, matplotlib, pandas, seaborn
- 3d force layout: vasturiano
- d3.js, impress.js